Corneal Crosslinking
Slowing Progression of Keratoconus
A newly FDA-approved procedure, corneal crosslinking is what we consider to be the mainstay of halting the progression of keratoconus. Corneal crosslinking is an accelerated means to structurally strengthen the cornea, which has the potential to slow or halt the progression of keratoconus. One interesting tidbit: The natural cornea becomes cross-linked over time, which means that, structurally, it becomes more rigid. It is the reason why a large subset of older keratoconic patients no longer progress—their cornea has naturally become cross-linked. Even though corneal crosslinking is an effective procedure to slow the progression of keratoconus, it unfortunately cannot reverse or cure the disease: it only slows or somewhat “freezes” the disease at its current state.
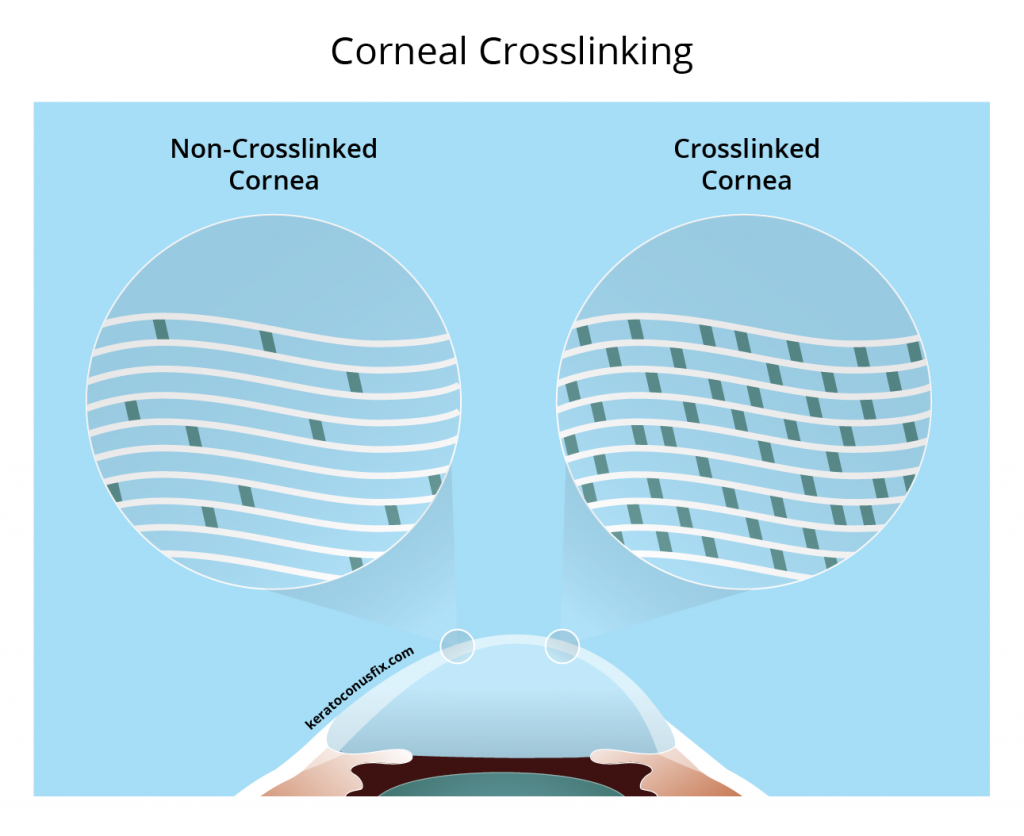
Corneal crosslinking is best utilized for younger patients who have been newly diagnosed with keratoconus, or for established keratoconus patients who are still progressing. This in-office procedure does not involve the removal of any tissue. Instead, a special solution is introduced to your eye, which is then activated with ultraviolet light, resulting in a more rigid cornea. Most patients do not experience a meaningful change in vision after the procedure as it is geared towards structural stability, not visual enhancement. Treatment goals involve stabilizing the cornea with corneal crosslinking then enhancing your vision with custom scleral lenses.
Implantable Intracorneal Ring Segments (Intacs)
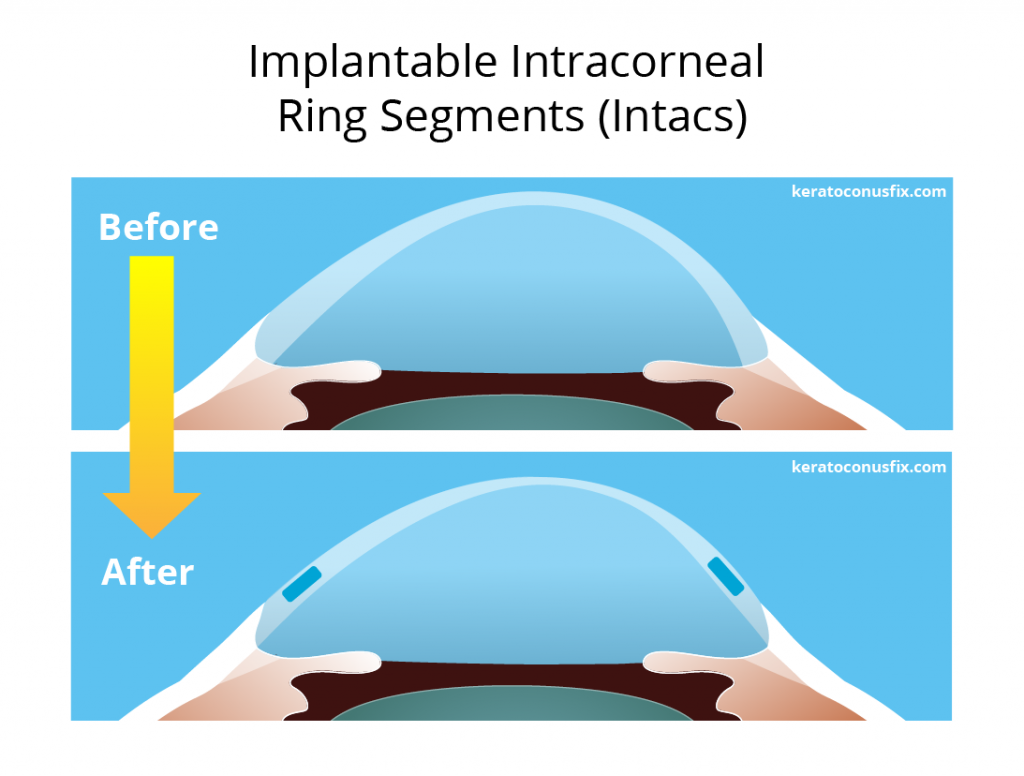
INTACS corneal inserts are a minimally-invasive, FDA-approved surgical option used to treat mild forms of keratoconus. With the natural disease course of keratoconus, the cornea bows forward as the structural fibers of the cornea weaken and thin. The forward-bowing aspect of the cornea results in a steeper cornea, which means that the healthy rounded shape of the cornea becomes more pronounced or cone-like (hence the name keratoconus).
INTACS solve to correct some of the steepness via structural relief. During this outpatient procedure, a surgeon creates a channel between the layers of the cornea, through which appropriately-sized, biocompatible rings are inserted. These rings bring structural relief to the cornea, reducing a portion of corneal irregularity from keratoconus. Under most circumstances, INTACS serve to reduce some of the resulting structural effects of keratoconus, but they do not slow the progression nor provide clear vision without the assistance of scleral lenses, contact lenses, or glasses.
Implantable Collamer Lens (ICL)
An ICL is a biocompatible contact lens that is implanted inside of the eye to correct for large amounts of myopia, also known as nearsightedness. More specifically, this lens is implanted between the iris (the colored aspect of your eye) and the crystalline lens (the non-visible lens that is tucked behind the iris).
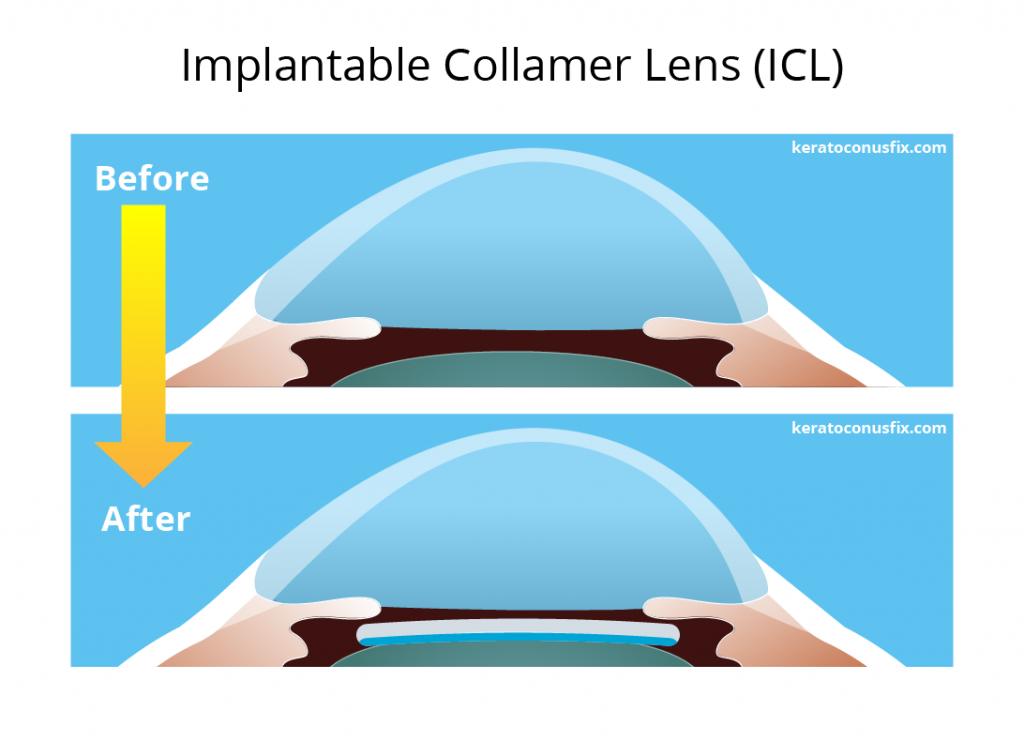
Your eligibility for ICLs is greatly dependent on a select number of critical factors. First, ICLs should only be attempted once your keratoconus has stabilized, which occurs only after elective corneal crosslinking procedure or with the natural aging process of the cornea. Second, your severity of keratoconus must be mild to moderate. ICLs are able to correct the majority of your nearsightedness, but they cannot correct the corneal distortion the overwhelming majority of patients with keratoconus have. The corneal distortion can only be remedied by wearing scleral or RGP lenses, which makes ICLs a less beneficial option for many.
Topography-Guided Photoreactive Keratectomy (TG-PRK)
TG-PRK is a non-FDA approved, laser-guided procedure that aims to reduce corneal irregularity and distortion that results from keratoconus. The standard form of the procedure, PRK, is similar to LASIK in that it is a procedure often used to correct nearsightedness and astigmatism in eyes without keratoconus. Standard PRK utilizes a guided laser that removes corneal tissue to arrive at or near a prescription of zero. With TG-PRK and patients with keratoconus, the endpoint is not a prescription of zero, as removing too much tissue will result in catastrophic thinning and weakening of the cornea. Instead, TG-PRK aims to remove the irregularities in the corneal surface that are responsible for visual distortion. Corneal crosslinking is necessary before attempting TG-PRK.
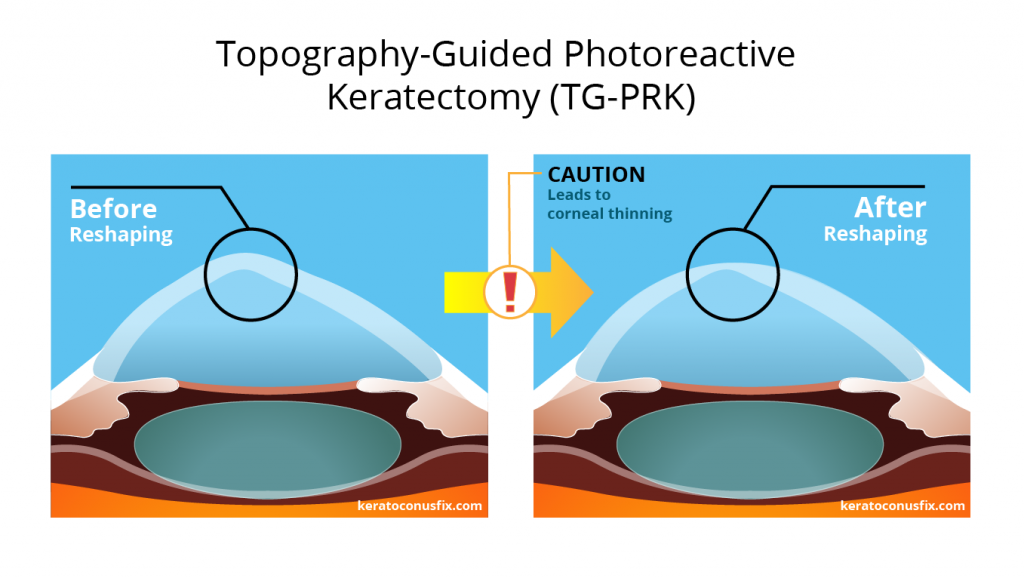
When evaluating options to treat your keratoconus, one must be cognizant of the effects of the treatment in the present and also the effects that might occur in the future. TG-PRK is a corneal subtractive procedure, which means that it utilizes a laser to remove tissue from keratoconic corneas that are already potentially thin. Even though the cornea-stabilizing crosslinking procedure is to be performed prior to TG-PRK, it is impossible to guarantee that keratoconus progression is 100% halted and that your cornea will not continue to thin. With even a small potential for minimal progression, our doctors do not believe that any corneal tissue should be removed from a patient with a corneal-thinning disease such as keratoconus.
Corneal Transplant
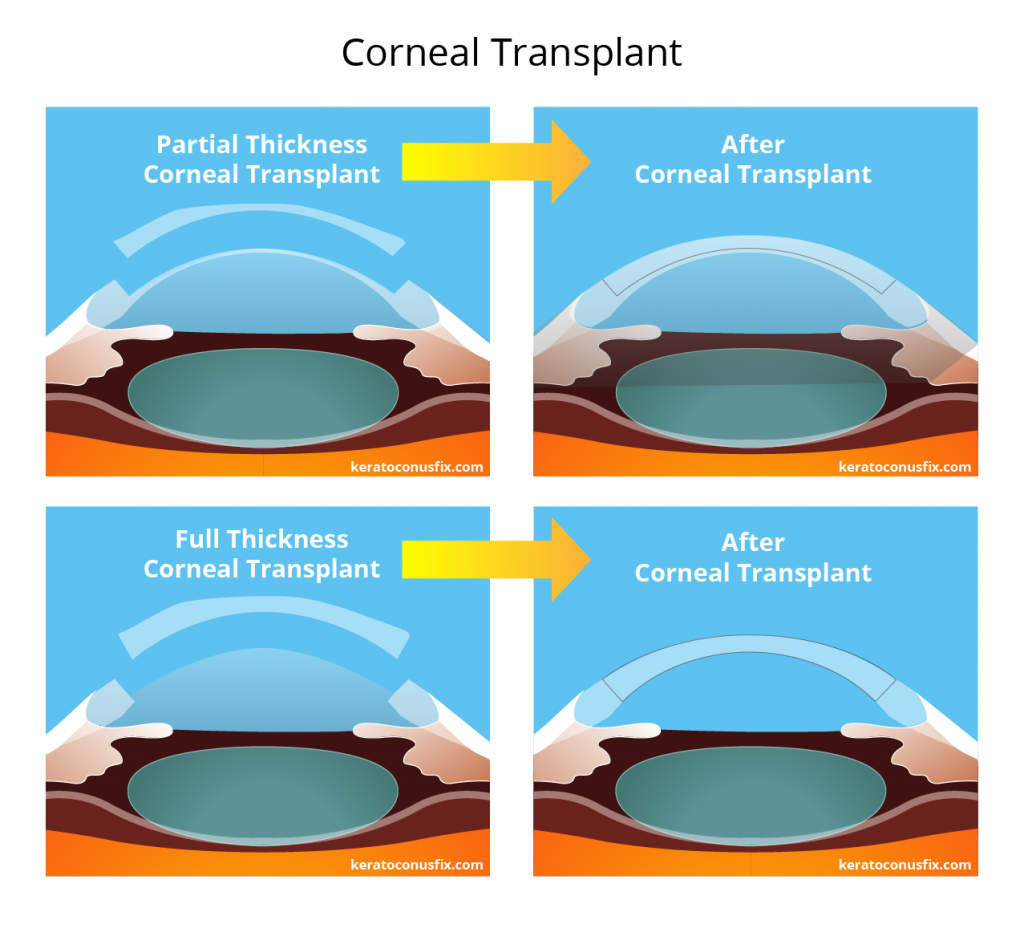
A corneal transplant is a surgical procedure that replaces damaged or scarred corneal tissue from keratoconus (in the context of this review). For the purposes of this discussion, we will be focusing on the newer form of the corneal transplant procedure, which is called Deep Anterior Lamellar Keratoplasty, aka DALK. With traditional “full thickness” corneal transplants, the entire depth of the central cornea is removed and replaced with a donor graft, which is then stitched into place. DALK differs from a traditional “full thickness” corneal transplants in that it is considered a “partial thickness” procedure. With DALK, only the damaged/scarred frontal half of the cornea is replaced. To illustrate the difference, consider how one can create a jack-o-lantern by carving a pumpkin. In creating a traditional top opening for your jack-o-lantern, you cut through the full thickness of the top of the pumpkin, creating a hole. With a DALK-like procedure, you would only cut partially through the top thickness of the pumpkin in creating a lid, so you never fully expose the internal of the pumpkin. With the partial thickness procedure, you leave much more of your structural and personal biological cornea intact.
In terms of visual performance, the replacement of a scarred cornea with that of a healthier donor cornea results in the potential for clearer, less distorted vision. It is unlikely that the donor cornea has the same optical prescription as the outgoing cornea, so glasses or contacts correction is required following a corneal transplant. Due to the nature of the stitches that are required to hold a donor cornea in place, scleral lenses offer the most comfort post-surgery as they can be designed to clear these stitches for the healthiest and most comfortable transition to clear vision.
Free Phone Consultation
Got more questions? Our experts are here to help.

References
Wagner H, Barr JT, Zadnik K. Collaborative Longitudinal Evaluation of Keratoconus (CLEK) Study: methods and findings to date. Cont Lens Anterior Eye. 2007;30(4):223-32.
One of the foundational studies evaluating 1,209 patients with keratoconus over a period of eight years. Its goals inclued characterizing the visual, anatomical, and quality of life changes due to keratoconus.
—
Barnett M, Ross J, Durbin-Johnson B. Preliminary Clinical Exploration of Scleral Lens Performance on Normal Eyes. JCLRS [Internet]. 22Nov.2018 [cited 6Dec.2018];2(2):e14-e21.
“According to participant surveys, scleral lenses were subjectively preferred over soft toric or gas permeable contact lenses in 88% of eyes…”
—
Cunningham B. Clinical Findings and Management of Pellucid Marginal Degeneration Using Scleral Lenses Over INTACS and Corneal Collagen Cross-linking with Riboflavin. JCLRS [Internet]. 19Jan.2018 [cited 6Dec.2018];2(1):e1-e14.
This case study provides an analysis of an individual affected by pellucid marginal degeneration (PMD). This particular case demonstrates the effectiveness of new scleral lenses over a severe form of PMD that underwent corneal crosslinking (CXL) with riboflavin over intra-stromal corneal ring segments (INTACS).
—
Gordon-Shaag A, Millodot M, and Shneor E. The epidemiology and etiology of keratoconus. Epidemiology 2012;70:1.
This review presents the scant epidemiological information known to date and the factors believed to cause the development of the disease.
—
Raiskup-Wolf F, et al. Collagen crosslinking with riboflavin and ultraviolet-A light in keratoconus: long-term results. J Cataract Refract Surg 2008;34(5):796–801.
“…results indicate long-term stabilization and improvement after collagen crosslinking. Thus, collagen crosslinking is an effective therapeutical option for progressive keratoconus.”
—
Davidson AE, Hayes S, Hardcastle AJ, Tuft SJ. The pathogenesis of keratoconus. Eye 2014:28:189–95.
In this review we summarise our current knowledge of the aetiology and risk factors associated with KC.
—
Jinabhai A, Radhakrishnan H, O’Donnell C. Pellucid corneal marginal degeneration: A review. Contact Lens Anter Eye 2011;34(2):56–63.
“Pellucid marginal corneal degeneration (PMD) is a rare ectatic disorder which typically affects the inferior peripheral cornea in a crescentic fashion. The condition is most commonly found in males and usually appears between the 2nd and 5th decades of life affecting all ethnicities. “
—
Schornack M, Patel S. Scleral lenses in the management of keratoconus. Eye Contact Lens 2010:1:39-44.
Jupiter scleral lenses provide acceptable visual acuity and comfort in patients with keratoconus. The availability of diagnostic lenses facilitates the fitting process. [Note, Jupiter lenses were one of the very first scleral lens designs]
—
Bromley JG and Randleman JB. Treatment strategies for corneal ectasia. Curr Opin Ophthalmol 2010;21(4):255.
“Early management of ectasia is essential to prevent its progression and to preserve visual potential. There are several management options that are available that may be used to reduce the need for corneal transplantation for these patients.”
—
DeNaeyer G, Sanders D. Collagen Crosslinking for Keratoconus Can Change Scleral Shape. JCLRS [Internet]. 28Mar.2018 [cited 6Dec.2018];2(1):e15-e21.
“Collagen crosslinking (CXL) for keratoconus is known to decrease, halt or even partially reverse progression of keratoconus. We report on a case where a substantial effect on scleral shape was also demonstrated.”
—
Hersh PS, Stulting RD, Muller D, et.al. United States multicenter clinical trial of corneal collagen crosslinking for keratoconus treatment. Ophthalmology 2017 Oct;124(10):1475–84.
To evaluate the safety and efficacy of corneal collagen crosslinking (CXL) for the treatment of corneal ectasia after laser refractive surgery.
—
DeNaeyer GD, Sanders DR. sMap3D corneo-scleral topographer repeatability in scleral lens patients. Eye Cont Lens 2017 Jul 21. doi:
The sMap3D measurements are repeatable with regard to scleral toricity and SAG values at a 16-mm diameter and thus would be suitable to use for scleral lens fitting.
—
Fadel D, Toabe M. Scleral Lens Hygiene and Care. JCLRS [Internet]. 24Apr.2018 [cited 6Dec.2018];2(1):e30-e37.
Scleral lenses (ScCLs) are developed using the same material as rigid gas permeable corneal lenses yet the care of scleral lenses differs from corneal lenses. These large diameter rigid gas permeable lenses necessitate hygiene, care and compliance protocol that is more complex compared with corneal lenses.
—
DeNaeyer G, Sanders DR, Farajian TS. Surface cover-age with single vs. multiple gaze surface topography to fit scleral lenses. Cont Lens Anterior Eye 2017 Jun;40(3):162–69.
To determine surface coverage of measurements using the sMap3D® corneo-scleral topographer in patients presenting for scleral lens fitting.
—
Craig JP, Nelson JD, Azar DT, et al. TFOS DEWS II Report Executive Summary. Ocul Surf 2017;15:802–12. 24. Alipour F, Kheirkhah A, Jabarvand Behrouz M.
Details the use of scleral lenses in moderate to severe dry eye.
—
Nau CB, Schornack MM, McLaren JW, Sit AJ. Intraocu-lar pressure after 2 hours of small-diameter scleral lens wear. Eye Contact Lens 2016;42:350–3.
Neophyte scleral lens wear of a 15-mm scleral lens for 2 hr does not increase IOP in healthy eyes. [Note, IOP refers to the internal eye pressure]